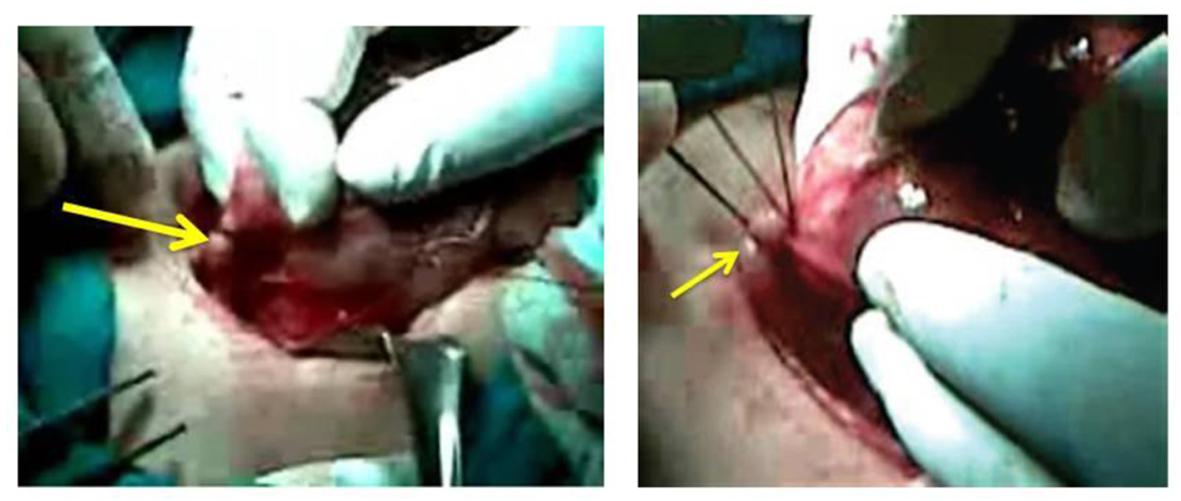
Figure 1. The superior thyroid artery indentified and dissected meticulously as close to the thyroid capsule as possible to avoid damaging the superior laryngeal nerve.
| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website http://www.currentsurgery.org |
Original Article
Volume 4, Number 2, June 2014, pages 40-45
Total Versus Subtotal Thyroidectomy for Benign Multinodular Goiter: Outcome and Complications
Figures

Tables
| Group | Permanent RLN injury | Temporary RLN injury | SLN injury | Total | P value |
|---|---|---|---|---|---|
| NS: not significant. | |||||
| ST (N = 121) | 0 | 3 (2.5%) | 3 (2.5%) | 6 (5 %) | NS |
| T (N = 121) | 0 | 4 (3.3%) | 3 (2.5%) | 7 (5.8%) | NS |
| Group | Permanent hypoparathyroidism | Transient hypoparathyroidism | P value |
|---|---|---|---|
| NS: not significant. | |||
| ST (N = 121) | 0 | 2 (1.6%) | NS |
| T (N = 121) | 1 (0.8%) | 1 (0.8%) | NS |