Figures
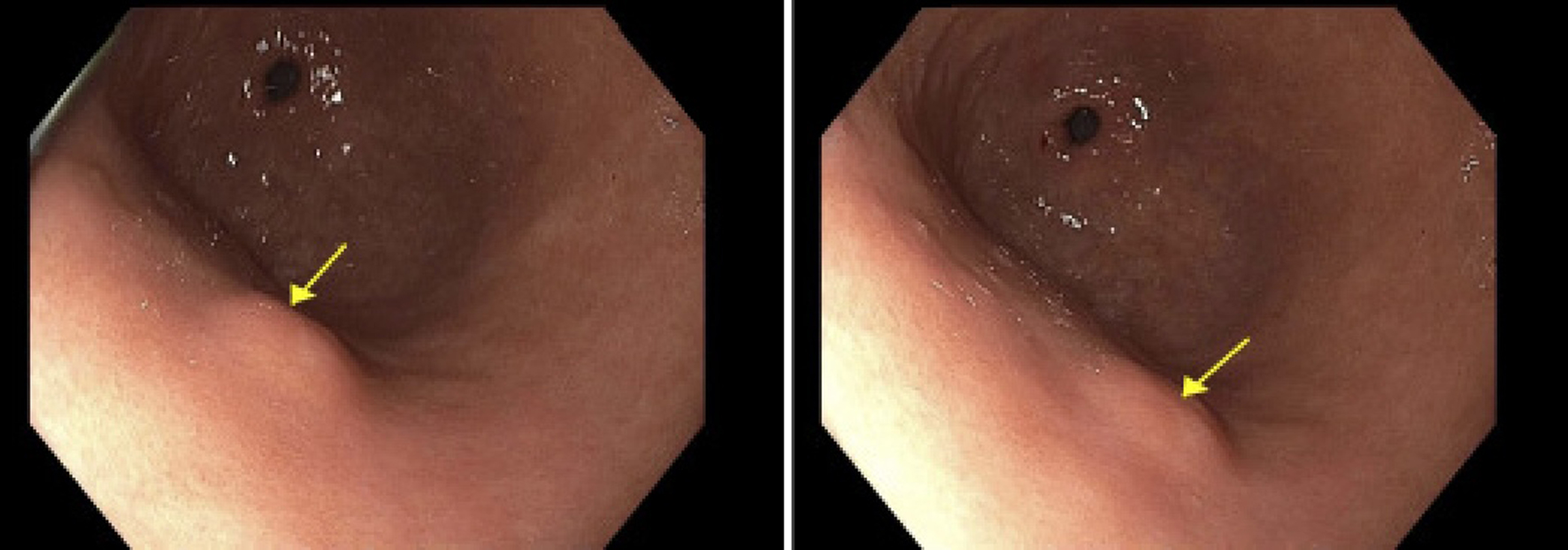
Figure 1. Endoscopic image showing a single 8 mm submucosal nodule (arrows) on the anterior wall of the gastric body. The lesion appeared hyperechoic on endoscopic ultrasound and invaded into the submucosa (layer 3).
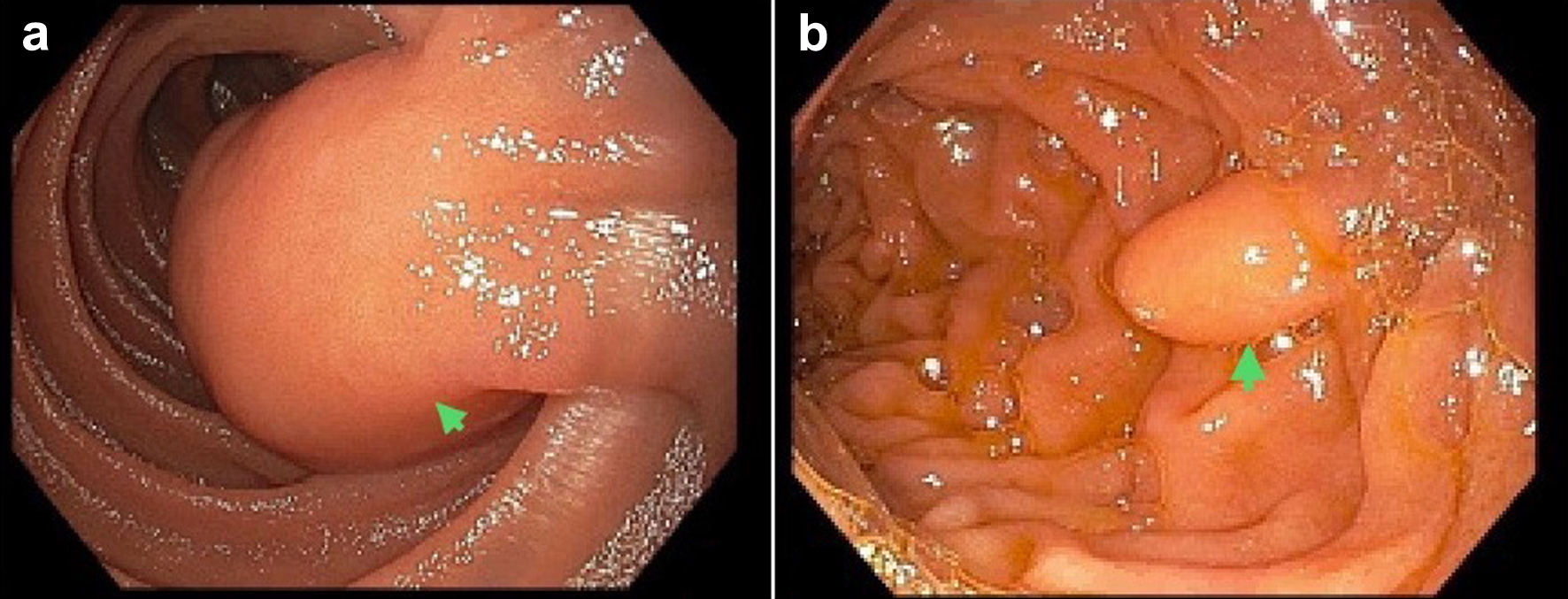
Figure 2. Endoscopic images illustrating lipomas in the small intestines. (a) A mass in the third portion of the duodenum (arrow). Histopathology was consistent with a duodenal lipoma. (b) A medium-sized lipoma, measuring 12 mm in diameter, in the second portion of the duodenum (arrow).
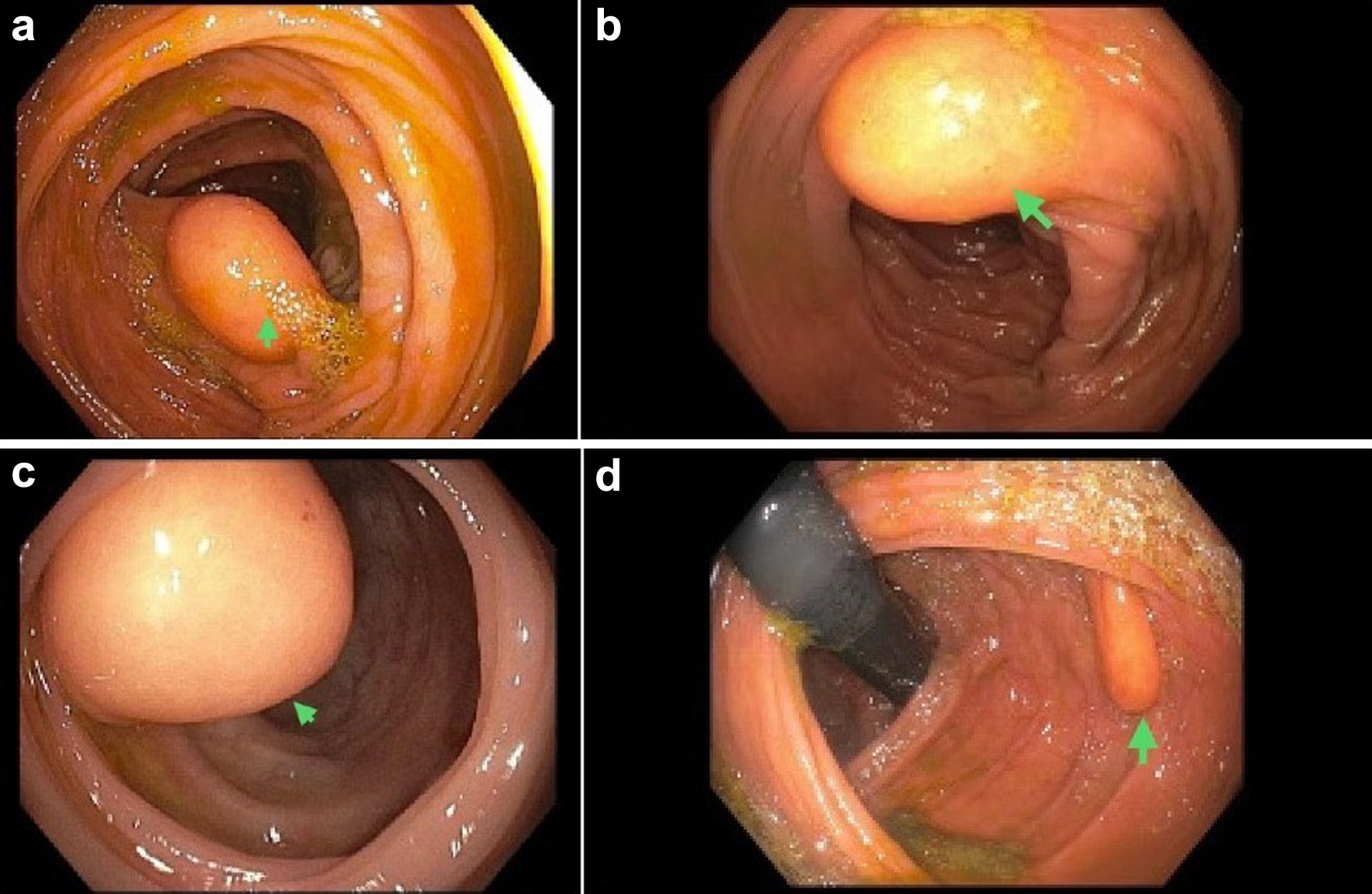
Figure 3. A library of endoscopic images showing colorectal lipomas. (a) A large lipoma, measuring 15 mm in diameter, in the ascending colon. (b) A medium-sized lipoma at the hepatic flexure. (c) A large lipoma at the ileocecal valve. (d) A medium-sized lipoma at the splenic flexure, in the transverse and ascending colon.
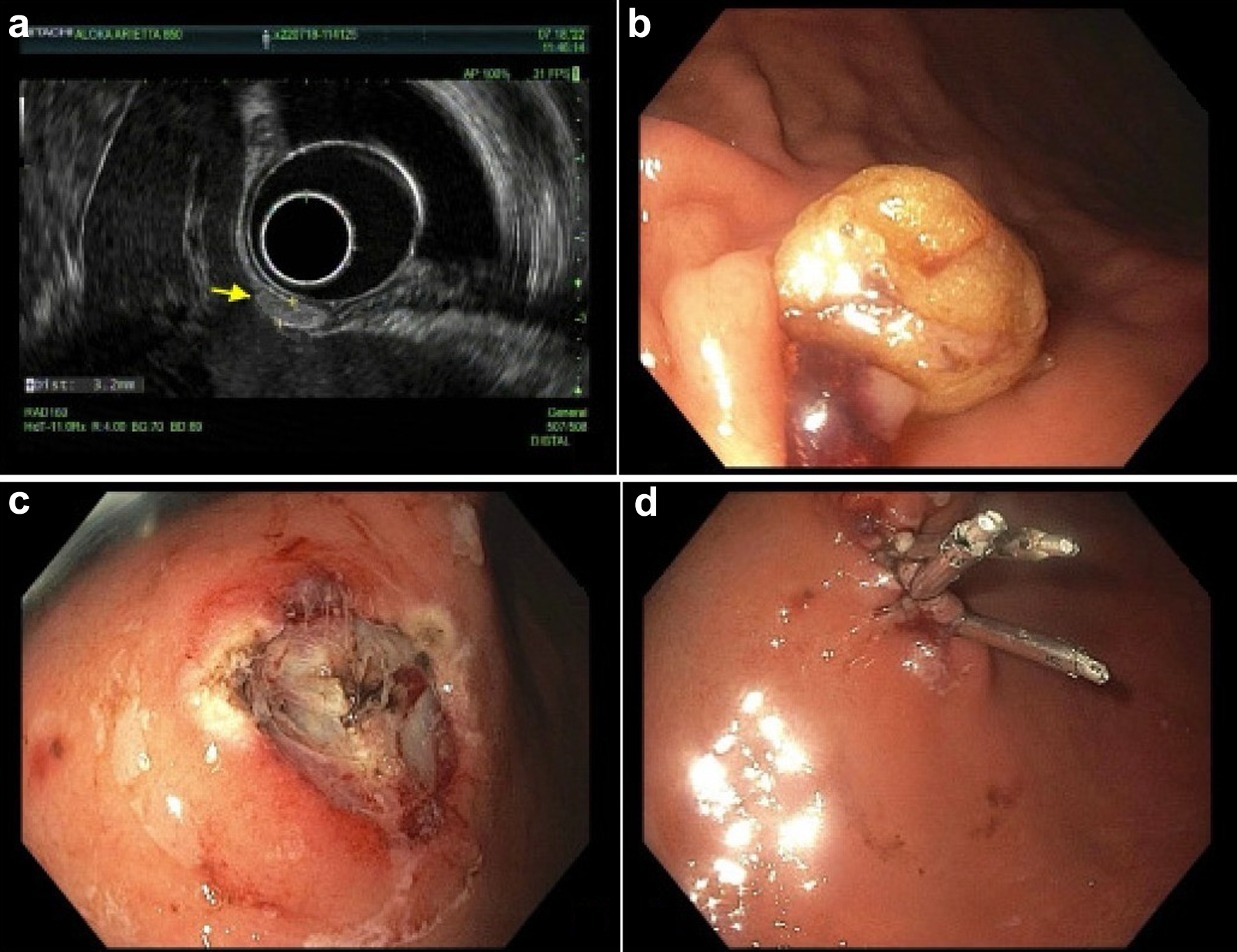
Figure 4. A library of endoscopy images showing the diagnosis and endoscopic mucosal resection of a gastric lipoma. (a) A hyperechoic oval nodule, measuring 3.2 mm in maximal cross-sectional diameter. There was sonographic evidence suggesting invasion into the submucosa. (b, c) A mucosectomy scar after mucosal resection of the lipoma. Three hemostatic clips were employed to close the surgical mucosal defect (d).